Comprehensive BLS Training & Certification for Healthcare Professionals in Stoughton, MA.
When a heart stops, seconds matter. This isn’t just about getting a certification card; it is about the physiology of perfusion, the precision of compressions, and the critical thinking required to save a life. Train with Nurse Practitioners who have managed real codes.
Status: Updated for 2025-2026 Medical Standards
Ideal For: Nurses (RN/LPN), Doctors, EMTs, Dentists, Pharmacists & Nursing Students.

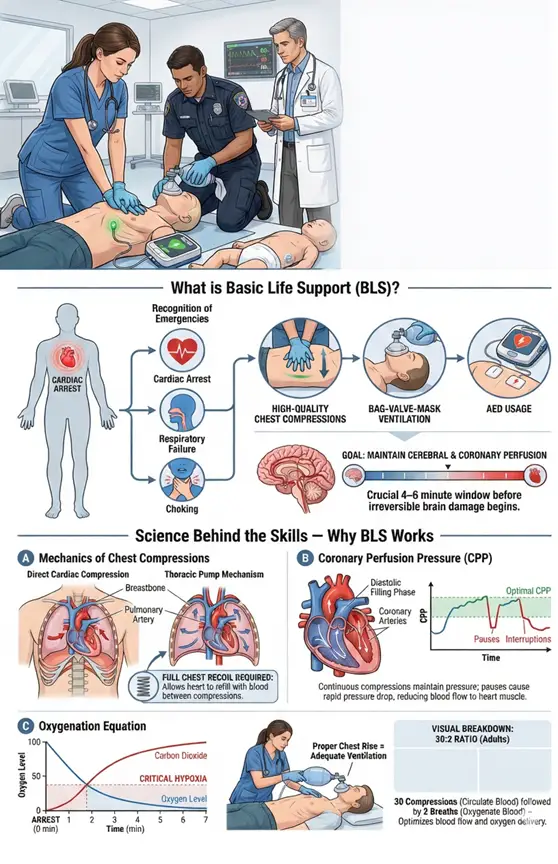
Basic Life Support (BLS) is the foundation of emergency medical care. Unlike standard First Aid which addresses minor injuries, or layman CPR which focuses solely on hands-only techniques, BLS is a systematic approach designed specifically for healthcare providers to sustain life during cardiac and respiratory arrest.
When cardiac arrest occurs, blood flow to the brain and heart ceases. Without intervention, irreversible brain damage begins within 4-6 minutes, and biological death follows shortly after.
life-threatening emergencies immediately (cardiac arrest, respiratory failure, choking).
Oxygenated blood to vital organs through high-quality chest compressions.
Patients effectively using barrier devices and bag-mask systems.
Shockable rhythms using an Automated External Defibrillator (AED).
To perform BLS effectively, a healthcare provider must understand why they are performing specific actions. It is not just pushing on a chest; it is manually taking over the function of the heart.
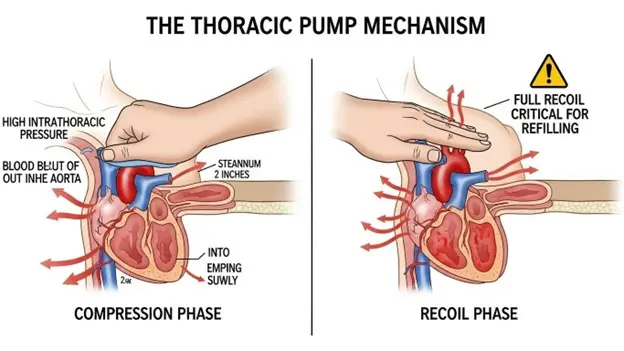
When you perform chest compressions, you rely on two primary mechanisms to move blood:
By pressing the sternum 2–2.4 inches deep, you physically squeeze the heart against the spine, forcing blood out of the ventricles and into systemic circulation.
Compressions increase intrathoracic pressure. This pressure gradient forces blood away from the chest during compression and pulls blood back into the heart during recoil (decompression).
This is why full chest recoil is non-negotiable. If you lean on the chest, you prevent the heart from refilling with blood. Compressing an empty heart generates zero blood flow.
The heart muscle itself needs oxygen to survive. During a normal heartbeat, the heart receives blood during diastole (relaxation). In cardiac arrest, the heart only receives blood during the recoil phase of CPR. High-quality BLS maintains Coronary Perfusion Pressure. If this pressure drops (due to pauses in compressions), the likelihood of a successful shock (defibrillation) drops significantly.
In the first few minutes of sudden cardiac arrest, the blood is still fully oxygenated. This is why compressions are the priority over breaths initially. However, as time passes, oxygen levels deplete.
True BLS competency goes beyond the basics. Here is the technical breakdown of the four pillars of survival we cover in our Stoughton, MA training center.
Before touching the patient, Scene Safety and Visual Survey occur simultaneously.
Tap and shout.
This must be done simultaneously in under 10 seconds.
A critical gap in training is recognizing Agonal Gasps. These are not normal breaths; they are reflex actions of a dying brain. Beginners often mistake this for breathing and stop CPR. Rule: If the patient is gasping and has no pulse, begin CPR immediately.
The difference between CPR and High-Quality CPR is the difference between life and death.
100–120 compressions per minute. (Too slow = low flow; Too fast = heart doesn't refill).
At least 2 inches (5 cm) for adults, but not more than 2.4 inches (6 cm).
Allow the chest to return to normal position after every push.
Minimize pauses to less than 10 seconds. Every time you stop compressing to check a pulse or swap rescuers, the blood pressure you built up drops to zero instantly.
Healthcare providers must use barrier devices to protect themselves and the patient.
Opens the airway for patients without trauma.
Mandatory technique for suspected spinal/neck injuries.
Requires a tight "E-C Clamp" seal. This is difficult for a single rescuer, which is why team dynamics are crucial.
For ventricular fibrillation (VF) and pulseless ventricular tachycardia (VT), CPR alone cannot restart the heart; it only buys time. An AED (Automated External Defibrillator) stops the chaotic electrical activity, allowing the heart’s natural pacemaker to reset.
Survival rates decrease by 7–10% for every minute defibrillation is delayed.
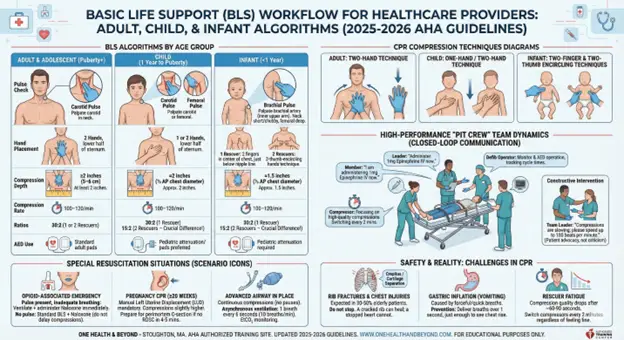
The physiology of a neonate differs drastically from that of a fully grown adult. Consequently, the approach to resuscitation must adapt. A “one-size-fits-all” approach can be ineffective or even harmful.
Here is the technical breakdown of how BLS modifications are applied based on patient age.
Accurate pulse detection is the first decision point.
Palpate the Carotid pulse in the neck.
Palpate the Carotid or Femoral pulse.
Palpate the Brachial pulse (inner upper arm).
The infant neck is short and chubby, making the carotid pulse difficult to find. The femoral pulse is often deep. The brachial artery is superficial and most reliable.
The mechanics of the pump change with the size of the chest.
| Feature | Adult | Child | Infant |
|---|---|---|---|
| Hand Placement | 2 Hands on lower half of sternum. | 1 or 2 Hands (depending on size) on lower sternum. | 1 Rescuer: 2 fingers in center. 2 Rescuers: 2-thumb-encircling hands. |
| Compression Depth | At least 2 inches (5 cm). | At least one-third AP diameter (approx 2 inches). | At least one-third AP diameter (approx 1.5 inches). |
| Rate | 100-120/min | 100-120/min | 100-120/min |
| Ratio (1 Rescuer) | 30:2 | 30:2 | 30:2 |
| Ratio (2 Rescuers) | 30:2 | 15:2 (Crucial Difference) | 15:2 (Crucial Difference) |
Children and infants rarely suffer from primary cardiac events (like heart attacks). Their arrest is usually respiratory in origin (choking, drowning, asthma). Therefore, they require more frequent oxygen delivery than adults. Switching to 15:2 doubles the ventilation rate.
In a hospital code or an EMS call, BLS is never a solo effort. “High-Performance Teams” use specific choreography to maximize blood flow and minimize interruptions.
A successful resuscitation team has clear, defined roles:
Focuses solely on high-quality compressions. Must switch every 2 minutes (5 cycles) to prevent fatigue.
Maintains the head tilt, seals the mask, and delivers breaths.
Operates the AED/Monitor and tracks cycle times.
Stands back (does not touch the patient), oversees the code, assigns roles, and makes treatment decisions.
Medical errors happen when commands are misunderstood. BLS protocols demand:
"Administer 1mg Epinephrine."
"I am administering 1mg Epinephrine." (Confirming the order)
"1mg Epinephrine administered." (Confirming the action)
If a team member sees a mistake, they must correct it immediately but respectfully.
If the compressor is slowing down, the Team Leader or Airway Manager should say: Compressions are slowing; please speed up to 100 beats per minute. This is not criticism; it is patient advocacy.
Healthcare providers often face scenarios that deviate from the standard algorithm.
With the opioid crisis prevalent in many communities, BLS providers must suspect overdose in patients with respiratory arrest.
If the patient has a pulse but is not breathing (or gasping), and opioid overdose is suspected, administer Naloxone (Narcan) immediately alongside rescue breathing.
Naloxone does not replace CPR. If there is no pulse, compressions take priority over medication.
Resuscitating a pregnant patient requires a modification to protect both the mother and the fetus.
The heavy uterus can compress the inferior vena cava, blocking blood return to the heart.
A second rescuer must manually pull the abdomen to the patient’s left side to relieve pressure, while standard compressions are performed.
Once an Endotracheal Tube (ET Tube) or Supraglottic Airway is inserted by an advanced provider, the 30:2 ratio stops.
Perform continuous compressions (do not stop for breaths).
Give 1 breath every 6 seconds (10 breaths/min) asynchronously. This maximizes Coronary Perfusion Pressure.
Most courses only show clean, sterile manikins. Real life resuscitation is chaotic, physically demanding, and visually disturbing. We prepare you for the reality.
Effective compressions require significant force. In elderly patients, it is common to hear or feel ribs cracking (crepitus) or cartilage separating.
A cracked rib can heal; a stopped heart cannot. Fear of causing injury is the primary reason for ineffective CPR.
If breaths are given too forcefully or too quickly, air enters the stomach instead of the lungs. This causes the stomach to distend and often leads to vomiting / aspiration.
Deliver breaths over 1 second, just enough to see chest rise. Do not hyperventilate.
Effective CPR burns a massive amount of energy. Studies show that compression quality (depth) starts to degrade after 60 seconds due to rescuer fatigue, often before the rescuer feels tired.
This is why the protocol mandates switching compressors every 2 minutes, regardless of how "fine" the rescuer feels.
The American Heart Association has released the 2025 Guidelines for CPR & ECC, and the changes are significant. If your BLS card is based on the 2020 guidelines, you are no longer current.
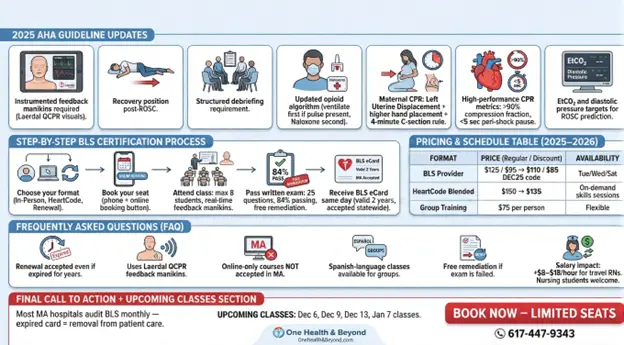
All BLS training MUST use real-time audio/visual feedback manikins. Courses without them do not meet AHA standards anymore. We use Laerdal QCPR manikins in every class so you can see your depth, recoil, and rate in real-time.
Particularly emphasized in opioid-related emergencies, unconscious breathing patients, and post-defibrillation stability.
Mandatory for clinical performance improvement and the emotional/psychological well-being of rescuers.
If pulse present, ventilate first, then give Naloxone. If no pulse, compressions take priority (Naloxone must not delay CPR).
Mandatory Left Uterine Displacement (LUD), slightly higher hand placement, and the 4-minute rule for perimortem C-section.
Compression fraction must be >90% and peri-shock pause <5 seconds.
Used for assessing CPR effectiveness and likelihood of ROSC.
Recommended for first-timers and hands-on learners.
Complete the online portion at home, then attend a 60–90 min skills session.
AHA eliminated the “initial vs renewal” difference. We honor the renewal price even if your card expired 3 years ago.
Use our booking link or call/text to reserve a slot.
Max 8 students per class, real-time feedback manikins, unlimited practice time. Skills check covers Adult CPR, Child CPR, Infant CPR, AED, and Bag-Mask Ventilation.
25 multiple-choice questions (84% required to pass). Free same-day remediation & retest if needed. (We maintain a near 100% pass rate.)
Valid for 2 years. Accepted by all MA hospitals including Mass General Brigham, UMass, Lahey, Steward, and Boston Medical Center.
Format | Regular Price | Dec 2025 Special | Availability |
BLS Provider (Initial/Renewal) | $125 / $95 | $110 / $85 (Code: DEC25) | Tue, Wed, Sat |
HeartCode Blended | $150 | $135 | Skills daily on demand |
Group Classes (10+) | $75 per person | – | We travel anywhere in MA |
Yes Laerdal QCPR with real-time depth/rate/recoil measurement.
No. An in person skills session is REQUIRED.
Yes for groups on request.
You receive free same day remediation and retesting. (Failure has never occurred in 4 years.)
Travel RNs earn $8–$18/hr more with active BLS. Many hospitals also restrict floating without current certification.
Absolutely. Most MA programs require BLS before clinical rotations.
Most MA hospitals now audit BLS status monthly. An expired card = immediate removal from patient care duties. Train with a DNP who has run real codes not someone reading off slides.
Or fill out our form → We respond within 5 minutes.